
I always thought “circuit breakers” caused unnecessary hardship and had no chance of nipping the problem in the bud, as their advocates claimed. It was criminal to not reopen the schools in June and I’m not entirely convinced they should be closed now. I scorn the likes of Piers Morgan and “Independent” SAGE who would have had us in lockdown all year if they’d had a chance. No amount of comparing Sweden to its immediate neighbours will persuade me that the Swedes didn’t have a better 2020 than most Europeans. Contrary to folk wisdom, you can put a price on life and it can’t be denied that most of the people who die of COVID have had a good innings.
I mention all this in the hope of establishing that I am not some wobbly-lipped pantry boy who’s scared of a bit of flu. I am a libertarian at a free market think tank who has spent most of his working life critiquing the excesses of the nanny state. I do not secretly harbour thoughts of creating a police state or bankrupting the economy.
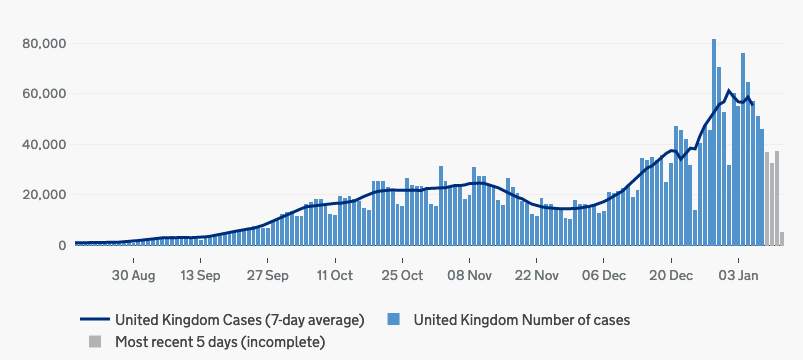
Nevertheless, I don’t think it is necessarily a bad idea to prevent tens of thousands of people dying this winter from a disease for which we now have multiple vaccines. I had hoped that we could muddle through with local restrictions, but the emergence in December of an extraordinarily infectious new strain put an end to that. The number of COVID cases doubled in the first half of December and doubled again in the second half. Much of London, Kent, and Essex seemed impervious to even the stringent tier 4 restrictions. We did not need a model from Imperial College to see which way this was going. In London and the south-east, there are now more people in hospital with COVID-19 than at the peak of the first wave. There are more on ventilators too, despite doctors using mechanical ventilation less than they did in the spring. It is going to get worse for some time to come. We had to get the numbers down.
I suppose my position is boringly centrist. If you want a more invigorating take, you might be drawn to the Zero COVID strategy supported by “Independent” SAGE or the plan laid out in the the Great Barrington Declaration to shield the vulnerable and achieve herd immunity the old-fashioned way. Both of these options carry significant downsides and have now been made redundant by the vaccines, but whilst these ideas might have been flawed or unrealistic, they were not crazy. The former had worked in New Zealand and the latter had been the preferred policy of the chief medical officer until the hasty U-turn of March 2020. These were ideas that reasonable people could debate without being considered cranks.
But now, in the final months of this nightmare, the conversation among many of the noisiest lockdown sceptics has become decidedly cranky. The debate unfolding on social media is not so much about how to deal with COVID-19 as about whether COVID-19 exists at all. Mention the latest official COVID statistics on Twitter and you will be inundated with replies from recently set up accounts telling you that the people who tested positive for COVID-19 do not actually have COVID-19 and those who are recorded dying from it probably got hit by a bus.
This would scarcely be worth worrying about if it were not spilling out into the real world. “Lockdown sceptics” have been recording footage of empty hospital corridors which they then post on YouTube as evidence that the health crisis is being manufactured. It saddens me to admit that this kind of thing is coming from people on my side of the argument, people who are anti-lockdown. Grifters, conspiracy theorists, and bad faith actors have been tolerated for too long by lockdown sceptics. You can draw a straight line from those who talked about a “casedemic” a few months ago to the crowds of protestors outside hospitals today screaming that “COVID is a hoax.”
Worked the late A&E SHO shift on NYE and came out to this. Hundreds of maskless, drunk people in huge groups shouting "Covid is a hoax", literally outside the building where hundreds are sick and dying. Why do people still not realise the seriousness of this pandemic? pic.twitter.com/KTkCtNf62A
— Matthew Lee (@mbklee_) January 1, 2021
Although debates about the lethality of the virus and the effectiveness of restrictions on social contact have been circulating on the margins since the spring, September was the point at which these talking points began to attract widespread attention. Ivor Cummins, a former Research and Development manager at Hewlett-Packard, first crossed my radar several years ago when he was promoting the low carb diet. At the time, he struck me as a relatively harmless nutritional entrepreneur with a mildly amusing name and a book to sell. He was an annoyance to scientists and dietitians who found his claims risible, but he was not a menace to public health. Cummins came to wider prominence on September 8th, 2020, when he published a 37-minute video entitled “Viral Issue Crucial Update Sept 8th: the Science, Logic and Data Explained!” In this presentation he claimed that “the epidemic largely ended around May/early June” and asserted that around 80 percent of Europeans were “already de facto immune” to the novel coronavirus. He claimed that increases in testing had created large numbers of false positives, leading to a “casedemic” in which the number of infections appeared to rise but there was “no mortality” because “the epidemic’s gone.” It attracted a million views on YouTube within days.
Cummins argued that the spring outbreak would have faded away naturally without non-pharmaceutical interventions such as lockdowns. Herd immunity, he theorised, had been largely achieved and he insisted that there would be no second wave. In the winter, he said, we would see “a natural rise in the virome [the combined total of viruses in the human body]; we’ll see influenza, we’ll see more impacts on hospitals, we’ll see SARS-CoV-2 rising again, but that will be more normal winter resurgent [sic] of influenza like prior years.” Cummins dismissed those who warned of a second wave in France and Spain, where case numbers were already growing, and described the rising caseload in the US as a “double hump” caused by the southern states experiencing their first wave. He assured viewers that the American spike was already on the wane. Within two months, France and Spain were recording more than 400 COVID deaths a day and the US was climbing its biggest “hump” yet, with every state except Hawaii experiencing uncontrolled community transmission.
Twelve days after Cummins’s video went viral, Michael Yeadon, a former Pfizer scientist, wrote an article for the Lockdown Sceptics blog arguing that the vast majority of positive tests for SARS-CoV-2 were false. If a test produces a non-trivial rate of false positives, he wrote, and if testing is performed at random on a population with a very low prevalence of a disease, it is possible for the majority—or even all—of the positive results to be false. Although he did not use the term, he was describing a familiar scientific concept known as the base rate fallacy. He was not wrong in theory, but he then went further. Based on the assumptions that 0.1 percent of the population had the virus and that the PCR test has a false positive rate of 0.8 percent, Yeadon made the striking claim that “almost every positive test, a so-called case, identified by Pillar 2 [testing in the community] since May of this year has been a FALSE POSITIVE. Not just a few percent. Not a quarter or even a half of the positives are FALSE, but around 90 percent of them.”
The mathematics were correct so long as Yeadon’s assumptions were correct, but they were not. People in Pillar 2 are not tested randomly. Many of them get tested because they have symptoms. People with symptoms are obviously more likely to have the virus than a random member of the public. The Office for National Statistics conducts a separate random weekly test which was reporting a prevalence rate of around 0.1 percent at the time. Strangely, Yeadon did not question the ONS figure and instead used it as the basis of his calculation. He did not draw the obvious conclusion that if the false positive rate of the PCR test was 0.8 percent, the ONS should find positives at least 0.8 percent of the time. Put another way, if every single positive test reported by the ONS was wrong—a far-fetched assumption—the false positive rate could not possibly be more than 0.1 percent. Moreover, the prevalence of SARS-CoV-2 in Britain was not low. Fewer than a thousand tests a day were coming back positive in July, but by the time Yeadon’s article appeared, they were exceeding 5,000. The number of tests performed each day had nearly doubled in this period, but that could not explain a fivefold increase in reported case numbers.
Yeadon’s concerns, which had always been largely theoretical, were now irrelevant and would become more so as the number of cases rose in the autumn. The claim that 90 percent of positive PCR tests are false was a back-of-an-envelope calculation based on flawed assumptions, but it was seized upon by COVID sceptics and given fresh impetus three days later when British foreign secretary Dominic Raab appeared on Sky News to explain why the UK was not testing inbound travellers at airports. “The challenge,” he declared, “is that the false positive rate is very high. It’s only seven percent of tests will be successful at identifying those that actually have the virus.”
Foreign Secretary Dominic Raab says the "challenge" with testing for #COVID19 in airports is 'the very high false positive rate' and adds 'only 7% of tests will be successful in identifying those who have the virus'.#KayBurleyhttps://t.co/7c8W5pWNmp pic.twitter.com/QG8EJnQbWH
— Sky News (@SkyNews) September 23, 2020
The clip duly went viral on social media but its central claim was totally implausible. Even Yeadon had only claimed a 0.8 percent false positivity rate. Although conspiracy theorists were convinced that Raab had accidentally let slip the truth, the mundane reality was that he had misunderstood the data on which he was relying. He was referring to a report by Public Health England which claimed that only seven percent of infected travellers would be identified through airport testing. This happened to be wrong. PHE made the hopelessly unrealistic assumption that infected travellers who were symptomatic enough to test positive would not get on a plane in the first place and that only seven percent would become symptomatic in the course of the flight.
Subsequent analysis by other academics found that testing at airports would identify between a third and two-thirds of cases, but that is not the main point here. The point is that PHE’s findings had nothing to do with false positives and Raab was wrong to use the phrase. If anything, he was talking about false negatives, but the COVID sceptics had Raab’s words in black and white and decided it was more likely that a widely used diagnostic test would have an insanely high false positive rate than that an unscientific politician would get his scientific terms mixed up during a live interview.
The false positive meme should have faded into obscurity by the end of October when more than 20,000 cases a day were being reported and the number of people in hospital with COVID-19 had risen tenfold. Instead, it became the foundation of an alternative theory of the pandemic. During the summer months, it had become tempting to believe that the pandemic was over, as both Cummins and Yeadon claimed, and that only a “casedemic” remained. Maintaining this belief in October, when the death rate had risen to a level last seen in May, took a certain amount of mental agility but a significant number of people were able to do it. The core ingredients of this alternative theory are as follows:
- The PCR test has a staggeringly high false positivity rate, meaning that the great majority of “cases” (the word is usually enclosed in derisory speech marks) are either asymptomatic or fake.
- Most of the people admitted to hospital with COVID-19 tested positive after they arrived, either because they caught the virus in hospital or because they were misdiagnosed with the unreliable PCR test.
- For the same reason, most of the people who are counted as COVID-19 deaths were admitted for treatment of another illness which killed them, or just happened to die within 28 days of testing positive (by one official measure, any death within 28 days of a positive test is classified as a COVID death).
- Lockdowns don’t inhibit the spread of the virus in any meaningful way and therefore do not reduce the COVID death count.
- Lockdowns cause a large number of avoidable deaths, not only in the longterm from unemployment, poverty, and missed cancer screenings, but also in the short term, e.g., from suicide.
So long as you believe these five tenets, you have a theory with almost impregnable circular logic. The acid test of the casedemic theory is whether the number of people being hospitalised and dying with COVID-19 increases after the number of positive tests increases. It clearly does, but true believers dismiss this as another mirage created by the false positives.
A rise in the number of excess deaths would be compelling evidence that the people dying “with COVID” had died of COVID and would not have died of anything else that year. The ONS has recorded excess mortality every week since mid-October, with the north-west hardest hit at first followed by London and the south-east more recently. In total, there were 71,731 excess deaths in England last year and 76,610 people had COVID-19 mentioned on their death certificate. Coincidence? Why yes, say the sceptics. They claim that the excess deaths were not caused by COVID-19, but by the lockdowns themselves. In any case, they say, the rate of excess mortality is lower than it was in the spring and the current rate is not without historical precedent. Any suggestion that there would have been even more deaths without lockdowns is dismissed as impossible because “lockdowns don’t work.”
With the delusions of September colliding with the reality of a second wave that will kill more people than the first, true believers have had to double down or flee the scene. Many have doubled down. Ivor Cummins, who once insisted that there could be “no second wave without a second virus” now claims that he “foretold the second wave” and has shamelessly accused governments of not preparing for it. Yeadon, who claimed in October that the pandemic was “over” in London and was “most unlikely to return” still insists that PCR testing is “wildly unreliable,” but has made his argument more technical so his lay followers have to accept it on trust.
As the HMS Casedemic slowly sinks into the ocean, the arguments used to keep it seaworthy stop making sense even on their own terms. COVID-19 has now killed more than 0.1 percent of the population in 20 countries, including Britain, but that has not stopped COVID sceptics claiming that the infection fatality rate (IFR) is 0.1 percent or lower. This would obviously require more than 100 percent of the population to have had the virus and is a particularly odd claim coming from sceptics who believe that most cases are false positives. Since the IFR is derived from the number of deaths and the number of infections, a lower number of infections would produce a higher IFR. Some sceptics believe that so few people have had COVID-19 that the IFR should be closer to 100 percent.
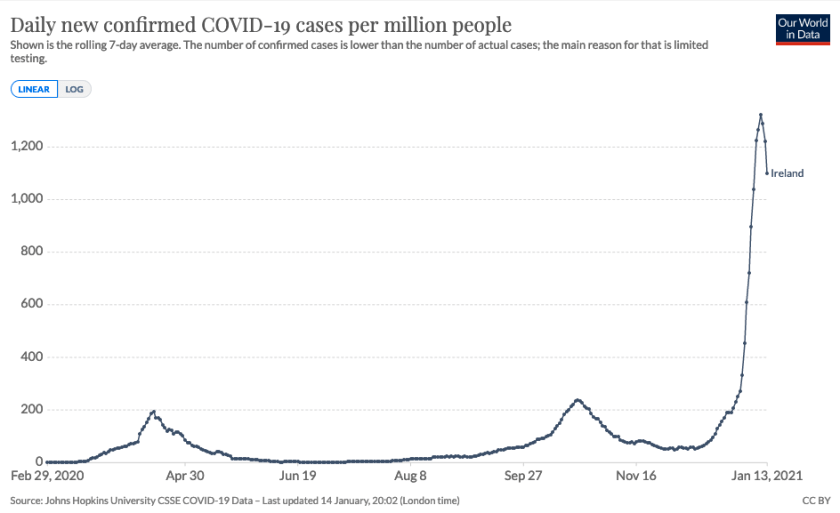
Cummins, who has raised over £148,000 to make a documentary about “one man’s remarkable rise to prominence as a ‘go to’ COVID commentator,” is having to perform a particularly difficult balancing act as he seeks to reassure his fans that the second wave of COVID-19 is nothing more than the normal “winter resurgence” of seasonal viruses that he predicted. His followers and subscribers seem not to mind his failed predictions and general inconsistency. Cummins recently suggested that the lack of excess mortality in Ireland last year was evidence that the panic over COVID-19 was overblown. Simultaneously, he has claimed that lockdowns in the UK have killed tens of thousands of people. Ireland spent longer in lockdown than the UK and yet the Emerald Isle seems to have mysteriously avoided the lockdown deaths that have supposedly plagued Britain. Ireland has also suffered far fewer COVID-19 deaths, but that cannot be explained by their lengthier lockdowns because—you guessed it—lockdowns don’t work.
If we define lockdowns as laws commanding people to stay at home except for essential purposes, the claim that they don’t work is either trivial or wrong. It is trivial if it meant to tell us that lockdowns merely push the problem into the future, and wrong if it is meant to suggest that they do not reduce the infection rate. As the standard of discourse has deteriorated, the latter interpretation has dominated.
The logic behind lockdowns is difficult to refute. If you reduce human interaction, you will reduce the virus’s ability to spread. In countries where mass testing is in place, you can see the effect very clearly. Within five to 10 days of a lockdown being introduced, the infection rate falls. A dramatic recent example is Ireland which went into lockdown on December 31st after seeing an almost vertical rise in cases. We saw the same thing in Wales in October and in England in November. In country after country, you can tell when a lockdown began by simply looking at the case numbers on a graph. Of course lockdowns don’t make the epidemic disappear and of course there are less restrictive policies that can reduce the caseload, but the claim that they don’t work at all is, to put it charitably, disingenuous.
In the heads-I-win, tails-you-lose world of the hardened denier, countries which lock down and have few deaths are proof that COVID-19 is a paper tiger, but if COVID-19 deaths fall after a lockdown comes into effect, the death rate was going to fall anyway because the virus was tired or herd immunity had been reached. In countries such as Britain which have managed to combine sporadic lockdowns with a high death rate, the claim is that the deaths are not due to COVID-19, but to the lockdowns themselves. And yet, if lockdowns are indeed the true cause of excess mortality, the COVID sceptics need to explain why there has been no excess mortality in countries such as New Zealand and Australia which introduced lengthy and draconian lockdowns and experienced very few COVID-19 deaths. They can’t. Nor can they explain why excess mortality has been highest in the regions of the UK that have had the most COVID-19 cases. And while they believe that people are dying at home because the NHS has been turned into a “COVID Health Service,” they cannot explain how creating more COVID patients is going to help on that front.
If tens of thousands of deaths have been wrongly attributed to COVID-19, then we are left to wonder what it is about testing positive for SARS-CoV-2 that makes people so much more likely to die within 28 days? Why are so many doctors recording COVID-19 as the main cause of death on death certificates if these people actually died of cancer or got hit by a truck? Why is the government using a diagnostic test with a 93 percent false positive rate and why isn’t that test producing false positives 93 percent of the time? And if lockdowns produce no appreciable health benefits, then why are governments voluntarily cratering their own economies for no reason?
The claims made by Cummins, Yeadon, and other supposed authorities are demonstrably nonsensical and yet they are eagerly lapped up by an army of social media disciples who have adopted the yellow smiley face as a badge of their scepticism. The smiley symbol is supposed to represent optimism in the face of adversity, but instead it makes the whole movement look decidedly cultish, creepy, and faceless, like the children in John Wyndham’s Village of the Damned. This disconcerting impression is reinforced by their tendency to say exactly the same things over and over again. Misleading graphs and blatantly doctored images are circulated with abandon, spreading far beyond the hub of hardcore believers and planting doubt in the minds of normal people.
Doubt is at the heart of this phenomenon, and it is being unscrupulously exploited. Can we prove that every death attributed to COVID-19 was caused by COVID-19? No. Some of them almost certainly weren’t. How many deaths were caused by lockdown? No one knows. Has the government ever specified precisely what the false positive rate is? No. Can we prove beyond doubt that the decline in case numbers seen around the world shortly after lockdowns were introduced would not have taken place anyway? No. How could we?
Some data simply don’t exist. Definite proof is only to be found in mathematics. In life, as in court, you can only exclude reasonable doubt. Those who cling to unreasonable doubts cannot be persuaded by facts or logic. The smiley crowd are persistent in asking questions about trivial issues for which there are no definitive answers, but have no answer to the most fundamental questions asked of them in return. Smileys generally won’t spell out the conclusion that their “scepticism” leads them to because they know how contemptibly stupid it would sound, but the scenario must go something like this:
A virus that has killed millions of people, including 50,000 in Britain last spring, suddenly disappeared, and so the government approved a highly inaccurate diagnostic test to keep the panic going because Boris Johnson has always wanted the public to wear face masks or something. Very few people actually have SARS-CoV-2 and even according to the official figures only two per cent have it at the moment. As luck would have it, a hugely disproportionate number of them happen to be admitted to hospital and die from something else, thereby producing scary death counts which are corroborated by corrupt doctors.
Another stroke of luck for the government is that last year happened to have the largest number of excess deaths since 1940. This could be due to lockdown deaths, whatever they are, or some other epidemic unrelated to the coronavirus. Have you noticed how few flu deaths there are this year? Bit suspicious, isn’t it? One possibility is that despite a drastic reduction in air travel and an unprecedented amount of social distancing, hand-washing, mask-wearing, and self-isolation, Britain is suffering from an exceptionally severe flu season, with flu deaths being wrongly classified as COVID-19 deaths by corrupt and/or incompetent doctors.
Pretty far-fetched, isn’t it? And that’s before we get to the theories about Bill Gates and the Chinese Communist Party that are on the lunatic fringes even in the smiley universe.
What is driving this insanity? Almost all COVID sceptics admit that there was a pandemic in the spring which killed tens of thousands of people in Britain. Why, then, is it so hard for them to accept the overwhelming likelihood that the same coronavirus is doing what viruses do and spreading rapidly in the winter? This is perhaps the most puzzling and interesting aspect of the whole phenomenon. The casedemic theory is just one of many daft ideas that have been thrown around in relation to COVID-19 in the last 12 months. Why has it not been quietly forgotten like so many others? How has it managed to survive, spread, and mutate with all the tenacity of the virus itself?
The answer, I think, lies in despair. Since March, there has been a sense of living in a nightmare from which one cannot awake. The non-pharmaceutical interventions introduced to contain the virus—especially lockdowns—have been soul-destroying. The economy is battered beyond belief, redundancies have gone through the roof, and there are more grey weeks of a cold winter lockdown to endure. On the other hand, we also have a potentially lethal and frequently debilitating virus infecting at least 50,000 people a day, hospitalising 4,000, and killing close to a thousand. That, too, will go on for weeks and, assuming you believe in germ theory and exponential growth, these figures would be much worse if we resumed normal social contact.
It’s an awful situation to be in. It’s a zero-sum game in which disease and death is traded off against misery and poverty. Until the first vaccine arrived in December, COVID scepticism offered people a way out. If the dangers of the virus were being overhyped by fearmongers, and lockdowns were entirely ineffective, then societies could reopen secure in the knowledge that there was nothing that could be done to reduce the death toll (which would, in any case, be a fraction of what we were told). The comforting lie that trade-offs could be avoided has proved irresistible to those who have surrendered to confirmation bias and constructed a parallel and preferable version of reality.
In this project, they have been ably assisted by the ignorance and statistical illiteracy that pervades Twitter. People who are not used to dealing with statistics have been trying to familiarise themselves with concepts and figures they’ve never seen before and don’t properly understand. Words and phrases are confidently repeated by those who don’t really know what they mean. There is no shortage of stupidity on Twitter, but this is something different, something almost transcendent. The inability to absorb or even acknowledge the most basic facts is beyond anything I’ve seen before.
But perhaps it’s not inability. Perhaps it’s just a refusal to face the reality of agonising choices. It is an extreme form of motivated reasoning, the flip-side to which is total credulity when presented with claims that suggest that there is no problem, no trade-offs, no pandemic, only malevolent governments and elites who could end the nightmare any time they wanted, but prefer to terrify their populations and needlessly wreck their economies instead.
We are in a no-win situation. The trade-offs are horrible. And so, when confronted by someone who tells you that’s it’s all fake, that the hospitals are empty and the test doesn’t work and the disease is basically harmless and the government is lying, who wouldn’t want to believe it? What could be more appealing than the idea that the thing we hate is causing the problem we’re trying to solve?
It would be nice if the hospitals were empty and the hundreds of thousands of people being infected each week were false positives. But we don’t live in that world, we live in this one. The smileys are not bad people. They are not necessarily unintelligent people. They are unhappy people wearing a mask of happiness, confused and beaten and searching for an easy answer. They want someone to flick a switch and make everything normal again. Who doesn’t? The trouble is that there are no easy answers this time.
Christopher J. Snowdon is head of Lifestyle Economics at the Institute of Economic Affairs and the author of Killjoys and Polemics. You can follow him on Twitter @cjsnowdon
A version of this article was originally posted at Quillette and has been reposted here with permission. Quillette can be found on Twitter @Quillette




























