But a new study may help explain some of the strangeness. Jeffrey Gold, M.D., and colleagues propose that the long-haul neurological effects of COVID arise from Epstein-Barr Virus (EBV), a ubiquitous member of the herpes family of viruses, being “turned on.” Although preliminary, the evidence is rather convincing.
Much like herpes simplex 1 and 2 (HSV-1 and HSV-2), which cause oral and genital herpes [1] EBV can be dormant and later reactivated, presumably by an immune stressor. Gold and his co-authors, writing in the journal Pathogens, provide the first evidence that brain fog, fatigue, and skin rashes that occur in 30% of people who have recovered from COVID can be correlated with EBV reactivation, which is a product of the COVID inflammatory response.
The evidence
According to Gold:
We ran EBV antibody tests on recovered COVID-19 patients, comparing EBV reactivation rates of those with long COVID symptoms to those without long COVID symptoms…The majority of those with long COVID symptoms were positive for EBV reactivation, yet only 10% of controls indicated reactivation.
Sidebar – Measuring reactivation
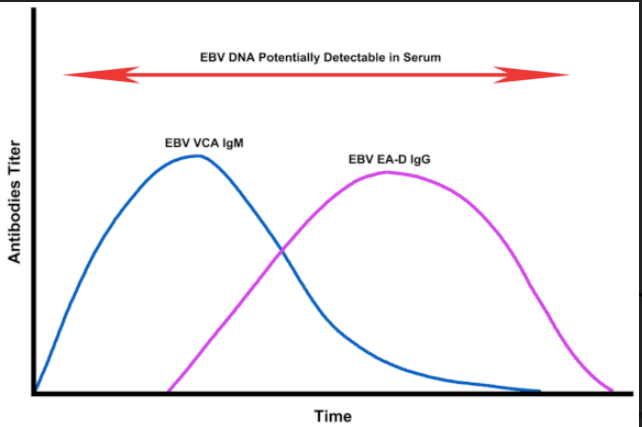
Measuring reactivation is straightforward. When herpes viruses reactivate and replicate, they form the viral components necessary to construct whole virions. These components, which are not present during periods of dormancy or chronic disease, can be measured. In particular, the EBV viral capsid antigen EBV VCA IgM is present in the early stages of EBV reactivation while another antigen called EBV early antigen-diffuse (EA-D) IgG (EBV EA-D IgG) found during chronic stages of the infection. A graphic from the paper (Figure 1) illustrates this:
Evidence
These findings suggest that many long-COVID symptoms may not be a direct result of the SARS-CoV-2 virus but instead the result of COVID-19 inflammation-induced EBV reactivation.
Gold’s group reported that:
- Of 185 randomly surveyed COVID patients, 56 (30%) developed symptoms of long COVID. This is a very scary number.
- A sub-group of 30 of the 56 patients was tested for the presence of EBV early antigen-diffuse (EA-D) IgG (indicative of EBV reactivation) or EBV viral capsid antigen (VCA) IgM (indicative of chronic disease).
- 20/30 (67%) of the patients had evidence of EA-D IgG. Only 2/30 had evidence of VCA) IgM
These findings suggest that many long COVID symptoms may not be a direct result of the SARS-CoV-2 virus but may be the result of COVID-19 inflammation-induced EBV reactivation.
– J. Gold, et. al.
What is the significance of these findings?
Since there are no effective treatments for EBV, the Gold study provides some understanding of the strange pathology of long COVID but does not point to any treatment for the disease at this time.
Notes:
[1] HSV-1 (“oral herpes “) is responsible for cold sores but is only too happy to cause genital lesions as well. HSV-2 causes genital herpes and is only a minor contributor in forming cold sores.Dr. Josh Bloom is Executive Vice President of the American Council on Science and Health. He has published more than 60 op-eds in numerous periodicals, including The Wall Street Journal, Forbes, and New Scientist. Follow him on Twitter @JoshBloomACSH
A version of this article was originally posted at the American Council on Science and Health website and has been reposted here with permission. The American Council on Science and Health can be found on Twitter @ACSHorg




























