Eleanor’s case was harrowing, but fortunately she didn’t need to be hospitalized. “I experienced overwhelming fatigue for much of the next ten days. I slept a lot. One night I got up and felt disoriented, hot and cold at the same time, and very unstable. I thought I wouldn’t make it to the bathroom or back to bed. I kept calling for Jesse, but he was sound asleep and never heard me.”
Fatigue and shortness of breath persisted. Scans revealed lung scarring, but Eleanor slowly recovered.
Through it all, Jesse never had a sniffle, cough, throat scratch or fatigue. Although he’d been beside his wife as the virus invaded her body for days, he never got sick. Later, his blood showed no antibodies against SARS-CoV-2, the virus that causes COVID. That meant that unlike people who are infected but then shake off the virus without getting sick, Jesse wasn’t infected in the first place.
Something was keeping the virus out of his cells so it couldn’t reproduce enough to show up on a diagnostic test or elicit an antibody response. Presumably a personal quirk of Jesse’s biology provided what experts call “inborn or natural resistance” to the pathogen.
Eleanor and Jesse are a “discordant couple,” one sick, one resistant. They and others like them hold the clues to developing antiviral drugs that block SARS-CoV-2 from entering our cells.
The COVID Human Genetic Effort
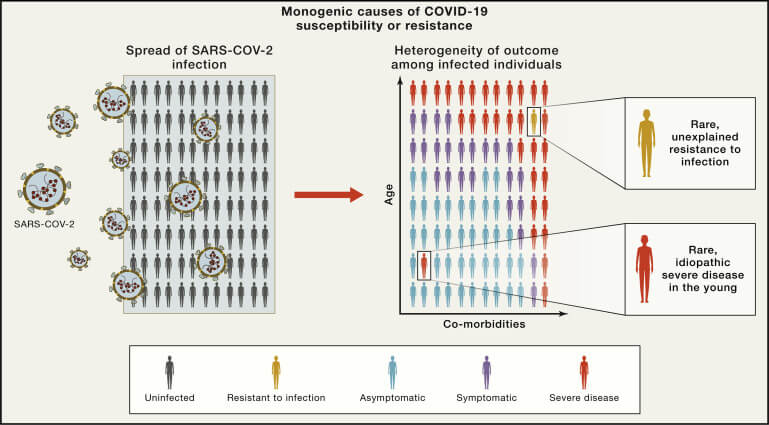
People who are naturally immune to COVID are the lucky owners of a variant of a gene that encodes a protein important in fighting off viruses. The COVID Human Genetic Effort is signing up these fortunate folks and drilling down on exactly how their gene variants – aka mutations – protect them. The researchers are looking first among genes that we already know account for the variability in how people experience COVID.
The project, “a global effort to dissect the human genetic basis of resistance to SARS-CoV-2 infection” is described in a recent report in Nature Immunology. The researchers are seeking 1,000 discordant couples. They’d already found 500 by the time the paper appeared, and soon after 600 more came forward. These special people will become a vanishing breed as vaccination masks discordant couples by preventing illness.
![]()
Many members of the COVID Human Genetic Effort team had already been investigating interactions of immune system proteins that could protect against viruses, like interferons and various receptors. I wrote about co-leader Jean-Laurent Casanova’s lab at the St. Giles Laboratory of Human Genetics of Infectious Diseases at Rockefeller University in 2013. Dr. Casanova, who speaks to the media about the genetics behind COVID, exemplifies the special group of researchers whose ongoing long-term work catapulted them instantly into the forefront of combatting the novel coronavirus.
Back in 2013, the goal of Dr. Casanova’s group was to identify single gene ‘holes’ in the immune defense that make otherwise healthy children highly susceptible to specific devastating, life-threatening infectious diseases. The flip side is people who are naturally protected and can’t become infected. To paraphrase the Borg (a collective of cyborgs) from the Star Trek universe, resistance, when it comes to COVID, is NOT futile. It provides information on how to better fight the enemy.
The COVID Human Genetic Effort is multi-focused, identifying and describing gene variants that:
- render infection impossible or undetectable
- rev up an immune response so rapidly that COVID symptoms never arise, despite infection (viruses entering cells)
- predispose a previously healthy person to develop severe COVID
Learning from past epidemics
History has inspired the COVID Human Genetic Effort, because clues to natural protection against infection have emerged before. For example, rare gene variants shield our red blood cells from malaria parasites and block the binding of noroviruses to our cells, making some people naturally immune to the “winter vomiting bug.”
A classic example of genetic protection is the CCR5 mutation. Cells of the one percent of people of European ancestry who have two copies of this mutation do not make complete receptors for HIV to dock on and enter human cells, and hence are resistant to HIV/AIDS. Understanding how these individuals evade HIV/AIDS, despite intense or repeated exposure to the virus, led to development of the drug maraviroc (Selzentry) to treat the infection in others. The drug blocks the receptors, mimicking a double dose of the CCR5 mutation.

Looking to history may also foreshadow a post-COVID world.
The population frequency of a mutation behind severe tuberculosis, for example, declined over 2000 years in Europe, as more people with the mutation died than those without it. That left fewer children to pass the gene variant on. The mutation disables an interferon, quelling the immune response to TB. Similarly, natural selection may weed out mutations that facilitate infection with SARS-CoV-2 as people of reproductive age succumb.
Seeking the resistant
A challenge in designing a scientific experiment based on real-world observations is in selecting individuals that share as many characteristics and experiences as possible. Constancy is critical to interpreting findings. Therefore, participants in the COVID Human Genetic Effort must be uninfected household contacts of sick people who were exposed for at least an hour a day without use of any personal protective equipment, during the first 3 to 5 days of the illness – such as people who sleep together like Eleanor and Jesse.
To be included in the study, the healthy partner must have tested negative four weeks after exposure to the virus. Then the researchers take over. They assess the T cell response, which is longer-lasting and more informative than measuring antibodies, which normally decline.
The mantra of immunity is that T cells command the B cells that mature into the plasma cells that crank out the abundant antibody proteins. The extreme variability of the receptors that dot T cells serve as name tags of individual immune responses. By assessing T cell receptors, researchers can discover exactly how people are naturally protected against specific infections. Antibody tests are used in large studies because they are much faster and cheaper to assess, but T cells indicate more lasting immunity.
If a potentially protected person – exposed but not sick – is negative on rapid antigen and PCR diagnostic tests and has no detectable antibodies or T cells against the virus, the next step in the COVID Human Genetic Effort is to sequence the genome. This genetic deep dive can reveal the specific gene variants that confer resistance.
And that’s where the work of another global consortium, the COVID-19 Host Genetics Initiative, enters the picture. They’ve been identifying human genes that affect how COVID unfolds since the pandemic began. When I wrote about the initiative a year ago, here and here, parts of the genome were just beginning to emerge as harboring genes that influence COVID susceptibility and severity. Today the image is sharpening.
Nailing down the genes that drive COVID susceptibility and severity — and possibly resistance
A first step in gene hunting is a genome-wide association study (aka GWAS), which compares patterns of SNPs (single sites in the genome that vary) that people with a trait share, like COVID severity. A GWAS is a little like people who love mysteries owning the same collection of books. Risk estimates derived from GWAS aren’t very strong, but they indicate where to look among a human genome’s 3 billion or so DNA bases for genes that confer a trait of interest.
A recent paper in The Lancet journal EBioMedicine propels the GWAS findings of a year ago a giant leap forward, closer to the genes behind the nuances of the COVID experience. The genetic clues of GWAS studies have evolved over the past year into more distinctive candidate genes that indicate COVID susceptibility and severity. Among these genes may also be variants that confer resistance.
Here’s a rundown:
- Chromosome 3: The short arm of this chromosome emerged drew attention early as housing genes that affect COVID because Neanderthal genes are in the vicinity too. The SLC6A20 gene encodes a protein that transports sodium and interacts with ACE2, the receptor on our cells for the virus. Variants of this gene reflect degree of susceptibility to COVID. Three other genes in this chromosomal neighborhood encode receptors that act like catcher’s mitts on the surfaces of T cells. A variant of one of the three genes, CXCR6, provides the strongest “severity signal” of the chromosome. Its encoded protein (a chemokine) recruits memory T cells to the lungs and is scant among COVID patients on respirators.
- ABO blood type: Evidence for a protective effect of type O blood and increased severity associated with type A has grown since a year ago, with 46 studies involving more than 50,000 people. Yet researchers are still trying to discover exactly how the blood type makes a difference.
- Interferon: Variants of the gene that encodes the receptor for interferon 1 are associated with critical illness from COVID and hospitalization.
- HLA variants: The human leukocyte antigens clustered on the sixth largest chromosome have been used to type tissues for organ transplants. Some of the 145 HLA combinations bind the virus and facilitate an antibody response better than others.
- ACE2: A gene on the X chromosome encodes the viral receptor, which festoons cells of the lungs, heart, kidney, digestive tract, and tissue linings. A study of more than 750,000 people through the UK Biobank and published in a preprint identifies a very rare variant that sharply reduces the number of ACE2 receptors on cells, which is correlated to a large decrease in risk of infection, but not to severity.
- Mucin: A variant of the mucin 5B gene known to lie behind the lung disease idiopathic pulmonary fibrosis is also associated with risk of hospitalization from COVID. That makes sense, because mucus provides an early defense against a virus.
- FoxP4: The gene forkhead box P4 encodes a transcription factor, which is a protein that affects the levels of a suite of other proteins. In healthy people, the functioning gene regenerates respiratory linings damaged from severe coughing and irritation. But a gene variant impairs the function enough to send COVID patients to the hospital, where often the lungs can’t rebound.
Genes and COVID: What are the data good for?
Throughout the pandemic, nurture seems to have trumped nature in terms of disease susceptibility and severity. In the lexicon of genetics, phenotype – the trait – trumps genotype – gene variants that cause or contribute to the trait. In practical terms though, emergency health care workers are going to treat a person’s symptoms ASAP, and not worry about genetic testing, which takes days for results.
A person with obesity, for example, faces increased risk of severe COVID whether the high body mass index arises from a genetic condition or from lifestyle. CDC’s list of medical conditions that raise risk of severe COVID includes illnesses with genetic and environmental components and causes, like lungs that are vulnerable from cystic fibrosis or from years of smoking.
Even though identifying gene variants that affect the immune response to COVID isn’t yet clinically useful, companies are already marketing tests to predict susceptibility and severity — but we’re simply not there yet, as several experts told Science magazine’s Jocelyn Kaiser.
I think that the more important genetic information is going to come from people like Jesse A., who inhale whopping loads of virus from their partners’ exhalations. What, exactly, protects them? The answers will inspire development of drugs that not only prevent COVID but also block even a toehold in the nose and throat, halting transmission too. By November of 2022, those gene candidates that have variants that offer resistance likely will have spawned drug candidates.
“No specific drug effective against COVID-19 has been discovered since the start of the pandemic. Lessons learned from experiments of nature could potentially guide us toward such specific treatments for COVID-19,” conclude the members of The COVID Human Genetic Effort.
Ricki Lewis has a PhD in genetics and is a science writer and author of several human genetics books. She is an adjunct professor for the Alden March Bioethics Institute at Albany Medical College. Follow her at her website or Twitter @rickilewis